
The ACL is the knee’s main front-to-back and rotational stabiliser. It has a poor blood supply and does not heal on its own, and around half of ACL tears occur alongside another injury. A torn ACL is reconstructed with a graft chosen around your sport, work, anatomy and goals — and the whole knee is inspected so a meniscus tear is repaired, not removed, at the same time.
What the ACL does
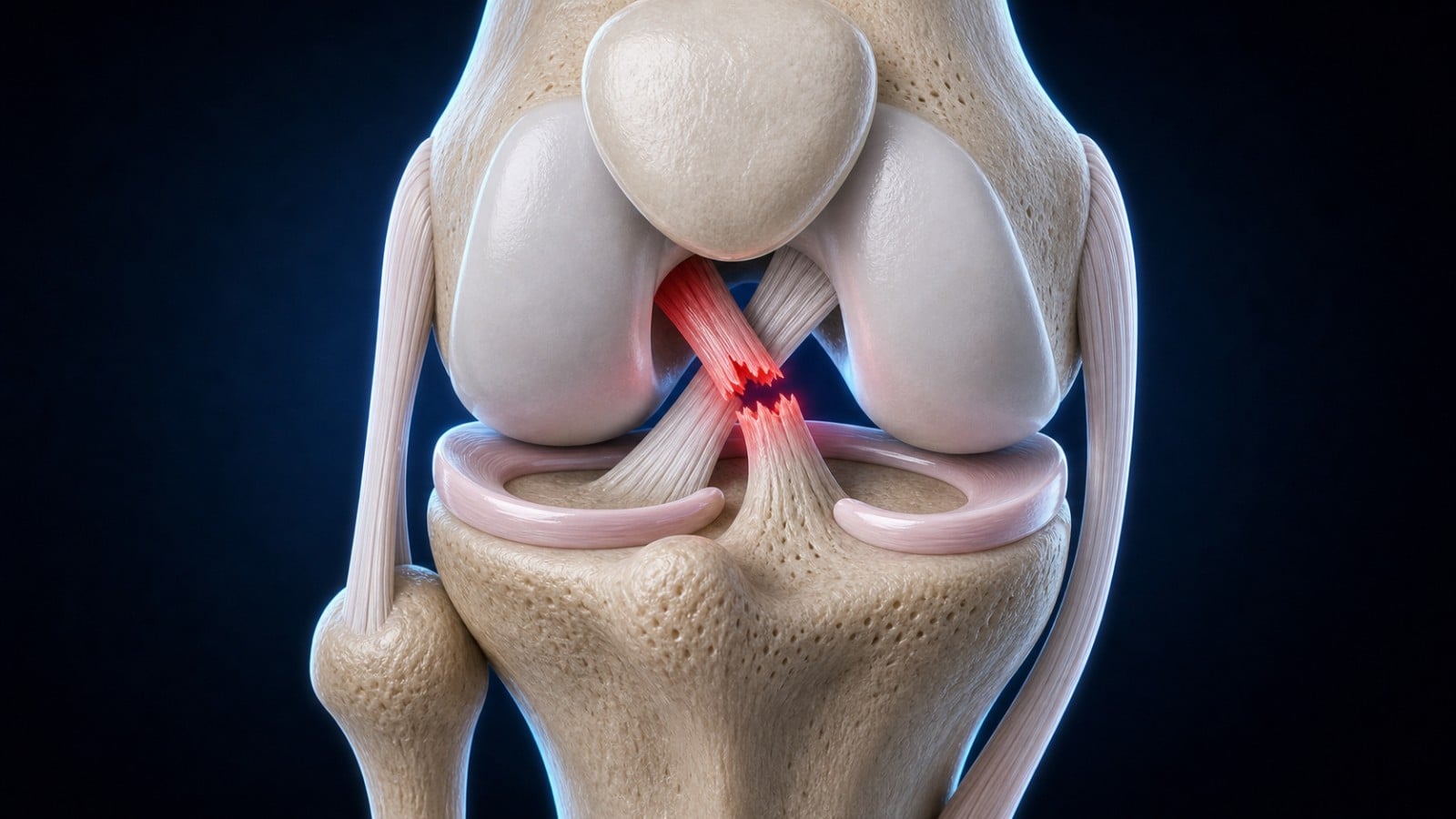
The anterior cruciate ligament (ACL) sits in the centre of the knee and is its main front-to-back and rotational stabiliser — it stops the shin bone sliding forward and twisting inward when you plant and turn.
It also protects the menisci, because a knee that keeps giving way grinds and tears them.

How it tears — and why it is not only a sports injury
About 7 in 10 ACL tears happen with no contact at all: a twist or pivot on a planted foot, an awkward landing, a misstep on uneven ground, or a slip off a kerb.
Many people feel or hear a "pop", followed by swelling within hours and a sense that the knee will give way on turning.
Why it matters
The ACL has a poor blood supply and does not heal on its own. Around half of ACL tears occur alongside another injury — a meniscus, the joint-surface cartilage, or another ligament — and a combined ACL-and-meniscus injury raises the long-term risk of arthritis.
This is why a torn ACL is assessed properly rather than simply rested.
How it is diagnosed
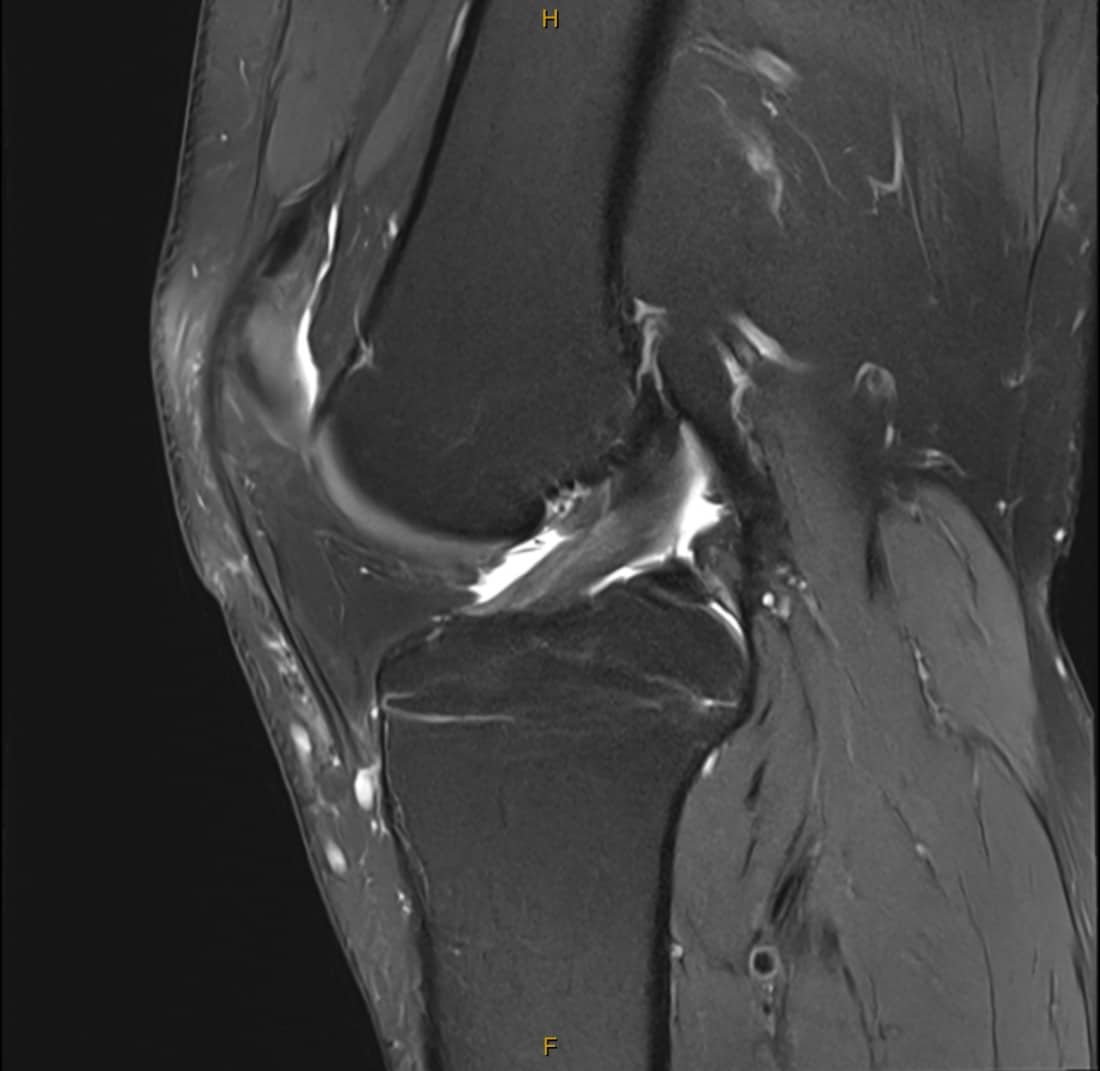
A careful examination (including the Lachman and pivot-shift tests) plus X-rays and an MRI, which confirms the tear and screens for the associated injuries that change the plan.
On an MRI scan, a healthy ACL shows as a clean, taut band of ligament running across the knee. When it ruptures, that band is lost — replaced by a gap and swelling where the ligament should be.

Graft options, explained clearly
A torn ACL is reconstructed (rebuilt with a graft), not stitched back together. There is no single "best" graft — the right choice depends on your age, your sport or work, your anatomy, and your goals. Dr Yas is trained and equipped to use all of the main graft options and selects with you, around your priorities.




“I am conversant with every graft option and the newest techniques, and I choose the graft around your particular priorities and needs — not a one-size default.”

Stylised illustration of a graft and fixation for explanation only — not an anatomically exact representation of your knee or implant.
Modern reconstruction
The defining principle is anatomic reconstruction — placing the new ligament exactly where your natural ACL sat. Mal-positioned tunnels are the single biggest cause of failure, so precise placement matters.
Surgery is arthroscopic (keyhole, day surgery for most), and the whole knee is inspected so any meniscus tear is repaired, not removed, at the same time.
When a previous ACL has failed (revision)
About 1 in 10 reconstructions fail — most often from tunnels placed poorly the first time, or a missed second injury (such as a posterolateral-corner or meniscus-root tear) that let the graft stretch.
Revision is more involved, sometimes staged, and is exactly the kind of complex problem other surgeons refer on.
Recovery and getting back
Rehabilitation is supervised physiotherapy and is essential. Return to pivoting sport is decided on your strength and control tests, not the calendar — returning too early raises the risk of re-tear. These are guides; many patients vary.




Guides to take home
Dr Yas’ own patient guides — plain-language, criterion-based and free to download. Your surgeon and physiotherapist will individualise them for your graft, any meniscus or cartilage work, and your sport.
Key takeaways
Common questions
Request a consultation
Send a few details and the rooms will be in touch within one business day.
Ask Dr Yas a question
Have a question about your knee? Send it through and Dr Yas’s rooms will respond. General information, not individual diagnosis.
Ask a questionLatest insights from Dr Yas
Plain-language articles on modern hip & knee surgery — written to help you make an informed decision.



- Beck NA, et al. ACL tears in school-aged children and adolescents over 20 years. Pediatrics. 2017;139(3):e20161877. (non-contact mechanism)
- Spindler KP, Wright RW. Anterior cruciate ligament tear. New England Journal of Medicine. 2008;359(20):2135–2142.
- MARS Group. Effect of graft choice on the outcome of revision ACL reconstruction. American Journal of Sports Medicine. 2014;42(10):2301–2310.