
The kneecap glides in a groove at the end of the thigh bone, kept on track by the groove’s shape, the MPFL ligament on the inner side, and the pull of the thigh muscle. When one of these is off, the kneecap drifts, catches or slips toward the outside — maltracking, and at its extreme, dislocation. Treating the cause early protects the cartilage.
The kneecap on its track
The kneecap (patella) glides in a groove (the trochlea) at the end of the thigh bone, like a train on a track. It is kept on track by the shape of the groove, a ligament on the inner side (the MPFL), and the pull of the thigh muscle.
When one of these is off, the kneecap drifts, catches, or slips toward the outside — this is maltracking, and at its extreme, dislocation.
Does this sound like you?
Many patients describe a lifetime of knee trouble: knock-knees, a kneecap that "gives way", a knee they cannot fully trust, and clicking or grinding at the front of the knee, worse on stairs or after sitting with the knee bent.
This is often patellofemoral maltracking — and it is very treatable.
Why treating it early matters
Each time the kneecap mistracks or slips, it can shear the cartilage on its underside. Left alone, maltracking grinds that cartilage and can wear the kneecap out at a young age (chondromalacia) — and once that surface is lost, it cannot be regrown.
Treating the cause early, before the cartilage is damaged, is far easier than dealing with the wear later. Two anatomical drivers — a shallow groove (trochlear dysplasia) and a high-riding kneecap — make slips more likely and are worth identifying.
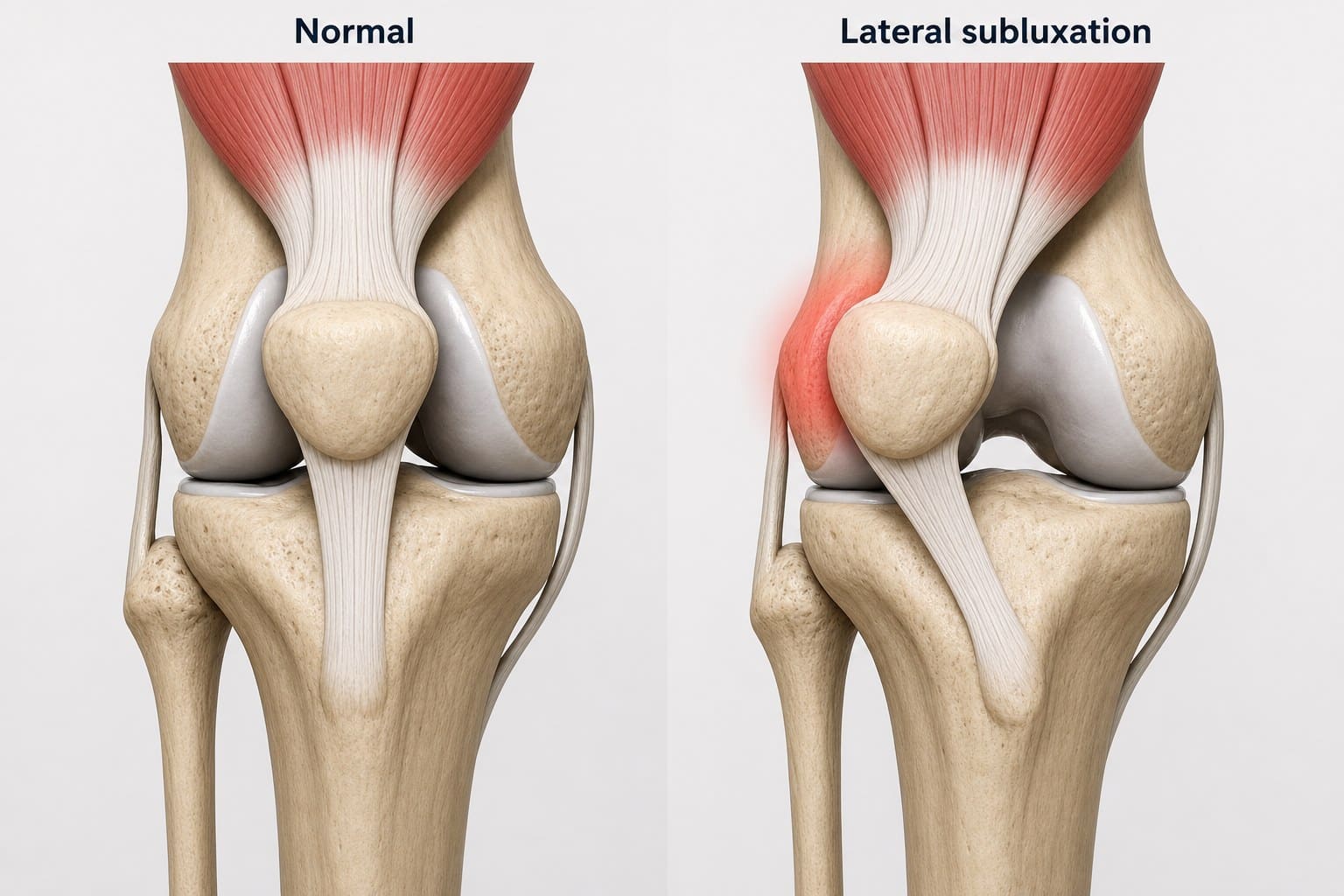
A normal kneecap sits centred in its groove; in lateral subluxation it slides toward the outer edge, straining the inner tissues. Stylised illustration.
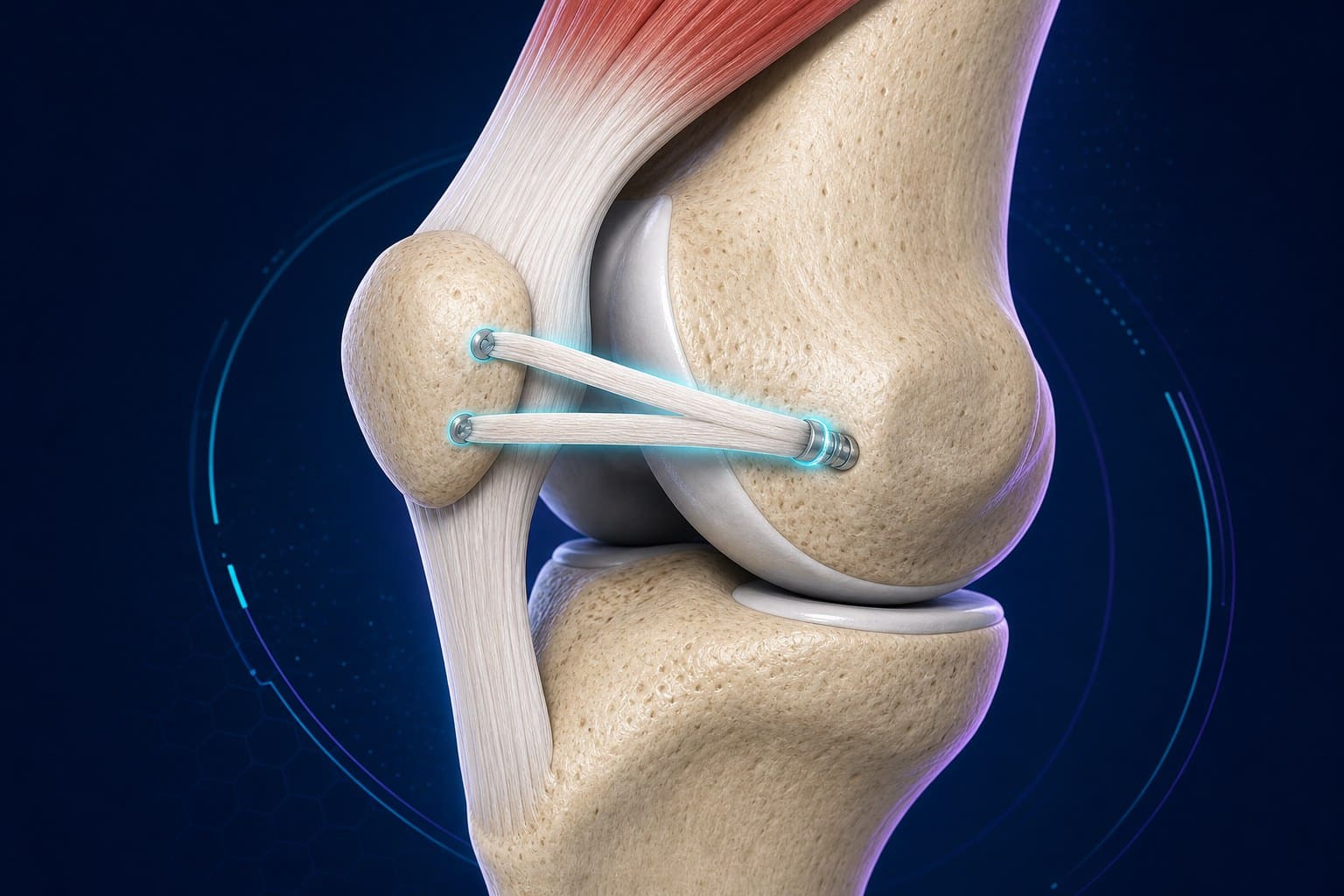
MPFL reconstruction: a graft rebuilds the ligament that holds the kneecap on its track. Stylised illustration.
Dr Yas’s solutions (keyhole and tailored)
Most first dislocations settle with focused rehabilitation.
When the kneecap keeps slipping, Dr Yas offers minimally-invasive, keyhole solutions tailored to the cause — rebuilding the inner ligament (MPFL reconstruction), and where needed realigning the pull of the kneecap tendon or addressing the groove — to stabilise the kneecap and protect the cartilage.
Key takeaways
Common questions
Request a consultation
Send a few details and the rooms will be in touch within one business day.
Ask Dr Yas a question
Have a question about your knee? Send it through and Dr Yas’s rooms will respond. General information, not individual diagnosis.
Ask a questionMore on knee injuries
Latest insights from Dr Yas
Plain-language articles on modern hip & knee surgery — written to help you make an informed decision.



- Fithian DC, et al. Epidemiology and natural history of acute patellar dislocation. American Journal of Sports Medicine. 2004;32(5):1114–1121.